How to Attract New Medical Graduates: Data-First Strategies for Modern Healthcare Recruiters
On this page
Related reading: Doccafe Vs Alpha Sophia What Healthcare Recruiters Need To Know, Attracting New Medical Graduates Strategies For Smart Healthcare Hiring, How Billing Data Helps Healthcare Recruiters Find The Right Providers Faster Smarter And With Fewer Surprises, Hospital, Healthcare Provider.
If you recruit physicians today, you’re working in the tightest market on record. The AAMC now projects a shortage of up to 86,000 doctors by 2036, a deficit driven by retiring baby boomers and an aging patient base.
Graduating residents feel that pressure every time they refresh their inbox. In the latest AMN Healthcare survey, 56% of final-year residents said they’d already received more than 100 job solicitations, while 78% logged at least 51.
Yet offers that lead with “competitive salary” land flat because priorities have shifted. 82% of residents rank lifestyle as “very important,” edging out the financial package they’ll take home.
Add a median medical-school debt of roughly $205,000, and hospitals now lose $7,000–$9,000 in revenue every day a seat stays vacant.
So naturally, the old spray-and-pray outreach model fails when every candidate is overwhelmed and every vacancy bleeds money. Winning teams move first with granular intelligence, knowing which residents finish in June, who grew up in a rural ZIP code, and whose visa clock is ticking.
Why It’s Harder Than Ever to Attract New Graduates
Six headwinds inflate competition and shrink your margin for error. Miss any one of them and the perfect candidate ghosts your pipeline.
Historic Supply–Demand Gap
Residency slots haven’t kept pace with retirements or population growth. Every six-month vacancy in gastroenterology wipes out roughly US $1.45 million in hospital revenue.
Chief-financial-officer data collected by Merritt Hawkins shows an average GI generates just over US $2.9 million per year, cut that in half for a half-year gap, and the seven-figure loss appears, even before you pay a dime for locum coverage.
Inbox Fatigue
Nearly four in five residents receive 51 or more job pitches, more than half cross the 100-message mark. Your first outreach arrives buried under a digital avalanche.
Lifestyle Over Location
In the same survey, 82% of residents ranked lifestyle “very important,” while only 4% said they’d practice in a community of under 25,000. If you lead with geography, especially rural geography, you’re already two squares behind.
Long Vacancy Clocks
MGMA benchmarking puts the specialty-average time-to-fill at about 8.4 months. Psychiatry, neurology, and critical-care roles often run longer. Every extra week drives up locum spend and patient leakage.
Cost of Churn
Replacing a single physician drains US $500 k–$1 M once recruiting fees, onboarding, and lost productivity are tallied. Hire wrong and you’ll pay that invoice again in 18 months.
Digital-Native Expectations
Gen Z doctors grew up tracking pizza deliveries in real time. They expect interview links, transparent comp grids, and text updates. Faxed credential packets mean prehistoric to them.
Data won’t erase these forces, but it can show where you still have leverage. That’s the pivot we make next.
Every US physician at your fingertips. Always.

Where Data Makes a Difference in Early-Career Recruitment
Data is not a spreadsheet, it’s actually leverage. Plug residency rosters, licensure files, and live engagement signals into an analytics layer (yours or a commercial tool), and each of the headwinds above becomes a dial you can turn.
Build a Living Resident Map
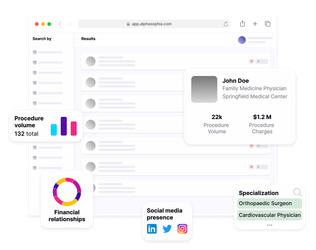
Merge NPI refreshes, GME rosters, licensure dates, and fellowship matches. In under a minute, you can surface every PGY-3 internal-medicine resident on an H-1B visa finishing in 2026, without doom-scrolling LinkedIn.
Nail the 90-Day “Yes” Window
Licensure timelines plus board-exam schedules reveal a 60- to 90-day stretch when each resident is most open to offers. One case study shows a hospital that timed its seven-on/seven-off pitch to that window and filled a psychiatry post in 90 days versus the 8.4-month norm.
Surface Lifestyle Clues Early
Pull call-schedule density from scheduling apps, moonlighting history from claims, and research interests from PubMed. A resident publishing on AI triage will ask about your data-science program. Another logging 18 overnight calls a month won’t be onboard without telehealth blocks.
Predict Rural Fit
Cross-reference hometown ZIPs, med-school states, and away-rotation sites. Graduates who have already spent time in similar communities are statistically more willing to return, which is crucial intel when only 4% prefer small towns.
Use that short-list, then sweeten it with loan-repayment stipends rather than ballooning base comp.
Watch Competitive Heat in Real Time
Track open rates on your emails and scrape public job board clicks (HIPAA-compliant). A sudden spike says the candidate is shopping for offers. Respond quickly with practical perks like flexible schedules, help finding a job for their spouse, or a clear path to leadership, before resorting to a higher salary.
Tie Spend to Impact
Dashboards that link cost-per-hire to vacancy days saved and projected billing make the ROI visible at a glance. Analysts calculate that every six-month vacancy in non-invasive cardiology results in approximately US $1.15 million in lost revenue, far more than the typical search-firm fee.
With these signals, you now know who to contact and when they’ll listen. The next section will turn that insight into outreach.
Personalizing Outreach That Builds Relationships
The inbox is your first impression, and data decides whether you get a reply. When every resident’s phone lights up with the same “competitive compensation” pitch, relevance is the only filter that matters.
-
Build a Single Candidate Profile
Workload clues: Pull night-call counts and moonlighting hours from scheduling feeds, anyone logging more than six overnight shifts a month is likely to value four-day blocks.
Visa & Family Data: Licensure files indicate H-1B status, and state teacher vacancies signal potential spousal job prospects.
Academic Signals: PubMed abstracts and recent poster titles tell you whether to highlight your data-science program or your rural loan-repayment fund.
Write One-to-One, Not One-to-Many
Emails with a personalised subject line are 26% more likely to be opened than generic blasts.
Keep the email to <90 words, close with a calendar link, and follow up by text inside 24 hours.
Use a Three-Touch Cadence Residents Can Fit Between Rounds
- Day 0 – Email: 90-word note pointing to a flex-schedule case study.
- Day 1 – Text: “Saw you opened, want a 10-min call after rounds?” Texts have a 98% read rate.
- Day 7 – LinkedIn DM: Share a resident-authored blog post your system recently published.
Once relationships start, you need a reason to invest long-term. That payoff is bigger than most CFOs realize. Next, we’ll see why this effort pays dividends far beyond the first contract.
Long-Term Value of Graduate Targeting
Hiring a resident is not a 12-month task, it’s a 30-year asset. Here’s why a data-driven graduate pipeline pays you back many times over.
A single six-month vacancy in a revenue-dense specialty erases more money than most sourcing budgets for the entire year. A hospital-revenue survey pegs annual downstream revenue at ≈ US $3 million for gastroenterology and US $2.3 million for non-invasive cardiology.
Halve those figures and you’re looking at US $1.4 million and US $1.15 million lost for every half-year the slot sits empty. That’s before you pay a dollar for premium locum cover.
But vacancy drag is only the front end of the ledger. Early-career retention multiplies the return:
Retention Economics
The AMA estimates turnover or burnout costs US $500 k–US $1 million per departing physician once recruiting fees, sign-on, and ramp-up losses are tallied.
A study adds that physicians who had finished residency or fellowship within the past six years stayed an average of “less than two years” in their first job, and the #1 reason they left was a mismatch with the practice’s ownership or governance model (cited by 35% of respondents).
Matching residents on factors like schedule, family fit, and visa support can spare you an entire churn cycle.
Referral Gravity
New primary-care hires feed every downstream service line. Industry revenue models show that an internal-medicine physician drives ≈ US $2.7 million to the hospital each year, as imaging, labs, specialist consults, and elective procedures follow their panel.
Lock that doctor in for a decade and you anchor well over US $25 million in cumulative billings, a stream no signing bonus can buy after the fact.
Leadership Pipeline
Residents who grow up inside your quality-improvement and telehealth protocols become tomorrow’s service-line chiefs. Promoting from within sidesteps six-figure executive-search fees and keeps institutional memory on campus.
Community Trust
Graduates who set roots raise their families locally, serve on civic boards, and mentor the next residency cohort, which is an intangible goodwill that lowers future recruiting friction.
When finance sees these compounding effects in a vacancy-versus-retention dashboard, the math is impossible to ignore. Trim just 90 days off a cardiology search and you recover nearly your data stack, recruiter hours, and a relocation stipend, with a margin left over.
That is why sourcing residents with precision data is less a hiring tactic and more a multi-year growth strategy.
Start Your Omnichannel Strategy with Alpha Sophia
FAQs
Why is it important to focus on new medical graduates in recruitment?
First-year physicians have the longest revenue runway. A single gastroenterologist, for example, contributes about US $2.9 million in net hospital revenue every year, capturing that doctor straight out of training secures decades of downstream income and referrals.
What challenges do recruiters face when targeting residents or recent graduates?
Competition is fierce, 56% final-year residents report receiving 100 or more job solicitations before graduation, so your message lands in a very crowded inbox. Lifestyle now trumps pay, as 82% rate “lifestyle” as very important, yet only 4% are willing to practice in towns under 25,000. Add a projected shortage of up to 86,000 physicians by 2036, and every graduate counts.
How can healthcare data help identify early-career HCPs more effectively?
Integrated datasets like GME rosters, NPI updates, licensure issue dates, scholarly output, and Open Payments, all together create a single, up-to-date profile for each resident. That view displays graduation timing, visa status, research interests, and even clues to burnout (e.g., excessive night shifts), allowing recruiters to target only those who genuinely fit the role.
What data points are most useful for segmenting new physician audiences?
Graduation year (PGY level) and licensure dates signal availability, J-1 or H-1B markers flag legal-support needs, call-schedule density and moonlighting hours reveal lifestyle priorities, home-ZIP distance highlights relocation propensity, scholarly keywords expose clinical passions, and engagement data (email or SMS opens) confirms active interest.
How can I personalize outreach to make it more appealing to recent grads?
Start with the subject line. Emails that include a recipient’s name or specific detail are 26% more likely to be opened. Keep the body to 90 words, reference something real, and end with a calendar link. Follow within 24 hours by text, making it the surest nudge.
Can Alpha Sophia help identify residents open to relocation or rural practice?
Yes. The platform scores relocation propensity by cross-matching hometown ZIP code, medical school state, prior rotation sites, and regional housing costs. Recruiters can filter instantly for “high-propensity” movers, vital intelligence when only 4% of graduates prefer small-town settings.
How early should outreach begin in a graduate’s training timeline?
Primary-care and hospital-medicine recruiters should start in PGY-2 so offers arrive before three-year programs finish. Competitive subspecialties often require 18–24 months of lead time because fellowship decisions are made early. Visa-dependent candidates benefit from an extra 3–6 months for paperwork.
What’s the long-term benefit of building a resident recruitment strategy?
Vacancy math is unforgiving: MGMA documents specialty searches that average 8.4 months, but flexible, well-timed offers have cut that to 90 days, restoring half a year of billable work. In revenue-dense specialties, a 90-day acceleration can recover roughly US $575 000 (half of the US $1.15 million lost during a six-month cardiology gap), and each avoided early departure saves another US $500 000–US $1 million in turnover costs.
Conclusion
Dashboards that match cost-per-hire to vacancy days saved make the value obvious. Even a 90-day faster fill in psychiatry, cardiology, or GI offsets platform fees several times over when the lost-revenue math is set beside the recruiting spend.
Data will never replace human rapport, but it does ensure that every conversation starts with the resident’s real priorities, like visa support, flexible scheduling, and research resources, instead of generic perks.
Marrying that precision with thoughtful outreach and new-graduate hiring stops feeling like a bidding war and becomes a long-term growth engine powering revenue, referrals, and future clinical leadership for the next decade and beyond.
